Box 1: Sample size calculation
Outbreaks of infectious diseases such as the 2019 novel coronavirus disease (COVID-19) pandemic have increased public awareness on behavioral modification as an important disease prevention strategy [1]. Although effective COVID-19 vaccines have been developed and recommended for use, they do not have 100% efficacy [2]. As a result, the most viable strategy for preserving community health amid the COVID-19 pandemic is the adoption of preventive behaviors through improved health literacy [3]. Health literacy has been described as the combination of abilities and skills needed to acquire, understand, and apply health knowledge in influencing health-related decisions [4]. Physical, traditional, and digital methods have been adopted to promote COVID-19 health literacy to contribute to disease prevention in both rural and local contexts [4].
It has been documented in the literature that rural dwellers face substantial health inequalities due to poor health resources, lower socioeconomic status, and low levels of education compared to urban dwellers in Nigeria [5]. Other population groups with a high likelihood of experiencing low health literacy include ethnic minorities, older adults, and those with compromised health status [6]. When compared with urban residents, rural residents have been described to have higher morbidity and mortality rates from cancer and cardiovascular disease [7]. A cross-sectional survey in Bayelsa State, Nigeria revealed a higher prevalence of poor health literacy among rural residents compared to urban [8]. Rural dwellers are not only disadvantaged in the allocation of healthcare resources, but also experience inequalities in the prevention and treatment of infectious diseases [9]. In the United States, it was found that mortality due to infectious diseases reduced by 18% between 1980 and 2014 with better indices reported in urban areas compared to rural areas [10]. Poor perception and knowledge of tuberculosis, hepatitis B virus, and the human immunodeficiency virus have been reported concerning rural residents in China [11]. Delay in the detection, reporting, prevention, and control of infectious diseases have been reported as unique challenges faced in both China and the United States [10,11].
The development of health literacy has become necessary to adequately prepare individuals and communities for the rapid containment of the COVID-19 pandemic and other unprecedented health events. Given that individual preparedness is key to solving real-life problems, enhancing health literacy is important to complement pandemic control efforts by government and citizens [11]. Good health literacy is required across rural and urban communities to ensure that community members are provided with quality health information and services to reduce their vulnerability to infectious diseases. This study therefore aimed to describe the pattern of COVID-19 health literacy in rural and urban communities in Nigeria.
This was a descriptive household-based cross-sectional survey conducted across rural and urban communities in Ondo State, Nigeria. Ondo State is one of the states in Southwest Nigeria, with its headquarters located in Akure city [12]. The boundaries of Ondo State include Kogi and Kwara States northward, Edo State eastward, Ogun and Osun States westward, and the Atlantic Ocean southward [12]. The official language of communication in Ondo State is English, which is frequently used in urban communities [12]. Yoruba language is the informal language of communication and is frequently used for informal communication. The economy of Ondo State is driven by agriculture.
Ondo State is one of the ten states with leading COVID-19 case reports in Nigeria. Of the 255,716 confirmed COVID-19 cases and 3,143 COVID-19 deaths in Nigeria as of 28th April 2022, Ondo State reported 5,173 laboratory confirmed cases and 315 deaths as of this reference date [13].
Individuals aged ≥18 years were recruited into this study from rural and urban communities of Ondo State. Due to the need for parental consent which may not have been available at the time of data collection, all individuals <18 years were exempted from this study. We included all individuals that showed willingness to participate in the study, and verbal informed consent was sought from each of them prior to administration of the questionnaire.
The sample size was calculated for this study using the sample size for comparing two proportions (Box 1) [14]. The minimum estimated sample size was 514. As the households in the communities existed in clusters, a design effect of 1.5 was used to increase the sample size. Thus, the calculated sample size for the study equaled 771.
We enrolled respondents from each community using a multi-stage sampling technique.
Stage One: Simple random sampling was used to select Akure South (urban) and Akure North (rural) local government areas.
Stage Two: Using the list of the political wards in each local government area as the sampling frame, four wards (sampling units) were selected from each local government area. Enumeration of the streets in each ward was conducted.
Stage Three: Using simple random sampling, a street was chosen from each of the selected wards.
A central location was determined by tossing a fair coin in each street. The direction corresponding to the head of the coin indicated the direction from which data collection would commence. All individuals aged ≥18 years were eligible for the study. Data collection continued until nearly one-half of the sample size was obtained from each settlement.
A structured interviewer-administered questionnaire was used for data collection. The questionnaire had three sections, namely:
Section A: This described the sociodemographic characteristics of the respondents, including age, sex, community type, level of education, living with people <18 years, health status (diseased or not), and wealth quintile.
Section B: This described the sources of COVID-19 health literacy among rural and urban community dwellers. The sources of COVID-19 health literacy included the World Health Organization (WHO), health workers, the Nigeria Centre for Disease Control, television, social media, newspaper, and COVID-19 hotlines.
Section C: Nine questions (on the ease of understanding COVID-19 information and ability to use the information correctly) were asked to determine respondents’ health literacy, each arranged on a scale of ‘1’ (very difficult) to ‘7’ (very easy). Using the Bloom’s cut-off set at 80%, good COVID-19 health literacy was defined as cumulative scores ≥50 points, and poor health literacy as scores <50 points.
Validation of the study tool was performed by infectious disease experts currently involved in the national COVID-19 outbreak response team in Nigeria. The questionnaire was pre-tested among 70 residents of communities that were not enlisted in this study, following which ambiguous questions were simplified. The questionnaire was translated to Yoruba and back translated to English language to ensure that the original meanings of the questions were preserved. Since nearly all the respondents had been enrolled in basic formal education, the questionnaire was administered in English language.
The predictor (independent) variables included the sociodemographic characteristics (already listed above), while the outcome (dependent) variables included sources of COVID-19 health literacy, proportion of individuals with good COVID-19 health literacy, and factors associated with good COVID-19 health literacy.
Data were collected by three research assistants who had obtained at least a secondary school certificate. The research assistants were trained on the mode and ethics of data collection. The training was conducted in both English and Yoruba languages on the 29th and 30th September 2020. A practical data collection session was organized shortly after the training to ensure adequate mastery of the data collection exercise in compliance with ethical principles. Data collection was conducted between the 1st and 30th October 2020.
Data were collected and input on the Statistical Software for the Social Sciences version 22 where data analysis was done [15]. Respondents’ ages were summarized using mean and standard deviation, while categorical variables were presented using frequency tables. The principal component analysis was conducted on the ownership of household items such as radios, televisions, stive refrigerators, electric fans, air conditioners, bicycles, motor vehicles, pipe-borne water, sewing machines, upholstered chairs, washing machines, and sewing machines. Results from the principal component analysis were arranged in quintiles: Q1 denoting the first (poorest) quintile, Q2 denoting the second quintile, Q3 denoting the third quintile, Q4 denoting the fourth quintile, and Q5 denoting the fifth (richest) quintile. To report the proportion of community members with good COVID-19 health literacy, we merged and reported the proportion of respondents that had selected options 6 and 7 for each source of COVID-19 information. Chi-square tests were conducted to assess the associations between health literacy and sociodemographic characteristics of the respondents. Variables that were significant in the bivariate analyses were pooled into the adjusted and unadjusted binary logistic regression models. The level of statistical significance was p <0.05.
Ethical approval for this study was obtained from the Health Research Ethics Committee of the Federal Medical Centre, Owo, Ondo State (Reference Number: FMC/OW/380/Vol. XCVI/75). This study was conducted in line with the Helsinki declaration [16]. Informed consent was obtained from each eligible participant, and each person was informed of their right to withdraw from the survey prior to its completion.
Overall, 691 community members responded to the survey for a total response rate of 90%. The median age of the 691 respondents was 27 years and ranged from 18-80 years. Among the respondents, 244 (35.3%) were aged 21-29 years and 160 (23.2%) were aged 30-39 years. Additionally, 352 (50.9%) were male, 407 (58.9%) had completed post-secondary education, 350 (50.7%) lived in rural communities, and 139 (20.1%) belonged to the fifth wealth quintile (Table 1). Among the respondents, 490 (70.9%) were willing to take the COVID-19 vaccine, while 229 (45.8%) had good COVID-19 health literacy.
Figure 1 describes the sources of COVID-19 health literacy among community members in Ondo State, Nigeria. Among the respondents, 409 (59.2%) obtained COVID-19 information from the WHO, 394 (57.0%) got COVID-19 information from health workers, 381 (55.1%) obtained COVID-19 information from the Ministry of Health.
Forty-eight (43.6%) adults aged ≤20 years had good COVID-19 health literacy compared to 72 (39.8%) aged 21-30 years, 45 (42.9%) aged 31-40 years, and 64 (61.5%) above 40 years (ᵡ2: 13.595, p = 0.004). One hundred and forty-three (49.7%) adults living in urban communities had good COVID-19 health literacy compared to 86 (40.6%) living in rural communities (ᵡ2: 4.062, p = 0.044) (Table 2).
Table 3 shows the urban-rural comparison of the association between COVID-19 health literacy and sociodemographic characteristics of residents in Ondo State, Nigeria. In urban communities, 36 (66.7%) adults older than 40 years had good COVID-19 health literacy compared to 35 (51.5%) aged 20 years and below, 50 (43.9%) aged 21-30 years, and 22 (42.3%) aged 31-40 years (ᵡ2: 8.995, p = 0.029).
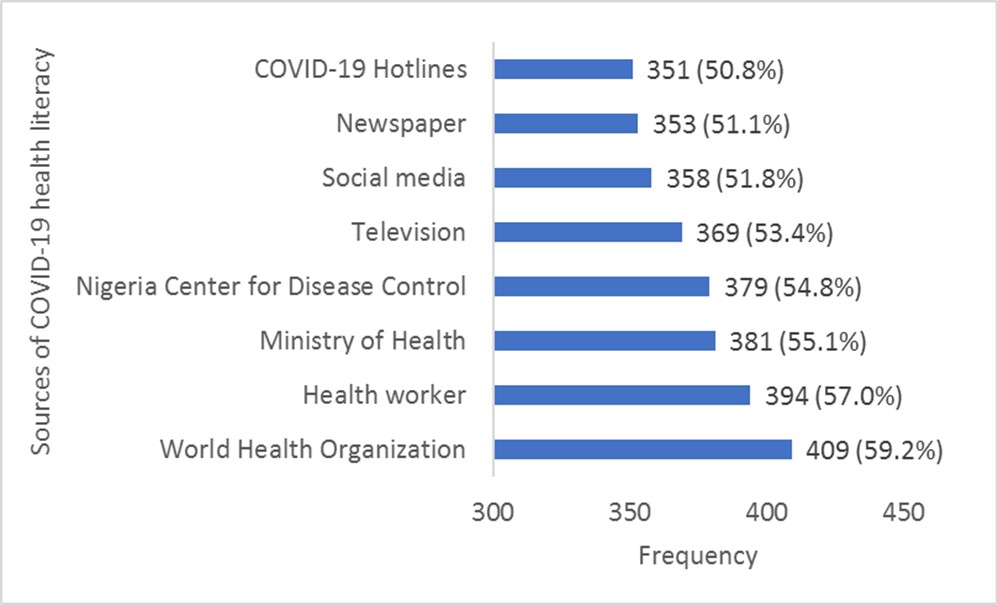
Sources of COVID-19 health literacy of the general adult population in selected urban and rural communities in Ondo State, Nigeria
In rural communities, 28 (56.0%) adults older than 40 years had good COVID-19 health literacy compared to 13 (31.0%) aged 20 years and below, 22 (32.8%) aged 21-30 years, and 23 (43.4%) aged 31-40 years (ᵡ2: 8.387, p = 0.039).
Table 4 shows the predictors of good COVID-19 health literacy among the general adult population in Ondo State, Nigeria. Adults aged >40 years had more than two times the odds of having good COVID-19 health literacy compared to those aged ≤20 years (AOR: 2.416, 95% CI: 1.373 - 4.253, p = 0.002). In addition, residents of urban communities were more likely to have good COVID-19 health literacy compared to residents of rural communities (AOR: 1.400, 95% CI: 0.971-2.020, p = 0.072).
In urban communities, people >40 years had nearly two times the odds of having good COVID-19 health literacy compared to those aged ≤20 years (AOR: 1.640, 95% CI: 0.769-3.495, p = 0.200). In rural communities, people >40 years had nearly four times the odds of having good COVID-19 health literacy compared to those aged ≤20 years (AOR: 3.523, 95% CI: 1.420-8.742, p = 0.007) (Table 5).
TABLE 4
Factors associated with good COVID-19 health literacy of the general adult population in selected communities in Ondo State, Nigeria
| Variables | Unadjusted Model | Adjusted Model | ||||||
| Unadjusted Odds Ratio | 95% Confidence Interval | p-value | Adjusted Odds Ratio | 95% Confidence Interval | p-value | |||
| Lower | Upper | Lower | Upper | |||||
| Age (Years) | ||||||||
| ≤20 | 1 | 1 | ||||||
| 21-30 | 0.853 | 0.528 | 1.379 | 0.517 | 0.887 | 0.544 | 1.449 | 0.633 |
| 31-40 | 0.969 | 0.565 | 1.662 | 0.908 | 1.105 | 0.636 | 1.921 | 0.722 |
| >40 | 2.067 | 1.197 | 3.568 | 0.009 | 2.416 | 1.373 | 4.253 | 0.002 |
| Community | ||||||||
| Urban | 1.445 | 1.01 | 2.068 | 0.044 | 1.4 | 0.971 | 2.02 | 0.072 |
| Rural | 1 | 1 | ||||||
| Wealth quintile | ||||||||
| First quintile | 1 | 1 | ||||||
| Second quintile | 0.781 | 0.455 | 1.342 | 0.372 | 1.26 | 0.732 | 2.169 | 0.404 |
| Third quintile | 0.952 | 0.55 | 1.648 | 0.86 | 1.104 | 0.635 | 1.92 | 0.726 |
| Fourth quintile | 0.631 | 0.363 | 1.096 | 0.102 | 1.543 | 0.885 | 2.687 | 0.126 |
| Fifth quintile | 0.439 | 0.247 | 0.779 | 0.005 | 2.277 | 1.279 | 4.052 | 0.005 |
TABLE 5
Factors associated with good COVID-19 health literacy among the residents of selected urban and rural communities of Ondo State, Nigeria
| Variables | Unadjusted Model | Adjusted Model | ||||||
| Unadjusted Odds Ratio | 95% Confidence Interval | p-value | Adjusted Odds Ratio | 95% Confidence Interval | p-value | |||
| Lower | Upper | Lower | Upper | |||||
| URBAN | ||||||||
| Age (Years) | ||||||||
| ≤20 | 1 | 1 | ||||||
| 21-30 | 0.737 | 0.403 | 1.346 | 0.32 | 0.789 | 0.428 | 1.451 | 0.445 |
| 31-40 | 0.691 | 0.334 | 1.431 | 0.32 | 0.69 | 0.33 | 1.441 | 0.323 |
| >40 | 1.886 | 0.901 | 3.949 | 0.093 | 1.64 | 0.769 | 3.495 | 0.2 |
| Live with a COVID-19 high risk group | ||||||||
| Yes | 3.779 | 1.566 | 9.116 | 0.003 | 3.108 | 1.255 | 7.693 | 0.014 |
| No | 1 | 1 | ||||||
| RURAL | ||||||||
| Age (Years) | ||||||||
| ≤20 | 1 | 1 | ||||||
| 21-30 | 1.091 | 0.476 | 2.5 | 0.838 | 1.238 | 0.523 | 2.93 | 0.627 |
| 31-40 | 1.71 | 0.731 | 4.003 | 0.216 | 1.98 | 0.817 | 4.801 | 0.13 |
| >40 | 2.839 | 1.201 | 6.71 | 0.017 | 3.523 | 1.42 | 8.742 | 0.007 |
| Wealth quintile | ||||||||
| First | 0.225 | 0.087 | 0.579 | 0.002 | 0.19 | 0.072 | 0.505 | 0.001 |
| Second | 0.708 | 0.314 | 1.595 | 0.404 | 0.531 | 0.225 | 1.252 | 0.148 |
| Third | 0.471 | 0.177 | 1.251 | 0.131 | 0.417 | 0.153 | 1.138 | 0.088 |
| Fourth | 0.49 | 0.216 | 1.113 | 0.088 | 0.373 | 0.158 | 0.883 | 0.025 |
| Fifth | 1 | 1 |
This study aimed to describe the pattern of COVID-19 health literacy in rural and urban communities in Nigeria. Findings from this study revealed that the prevalence of good COVID-19 health literacy was higher among urban dwellers (49.7%) compared to rural dwellers (40.6%). A cross-sectional study on urban-rural differences in COVID-19 preventive behaviors in China found that rural dwellers had lower tendencies to correctly process COVID-19 information compared to their urban counterparts [17]. A community-based cross-sectional study of 2,999 individuals conducted in Abia State, Nigeria reported the prevalence of better health-seeking behavior among urban residents compared to rural residents [18]. In another cross-sectional study among 763 migrant, 459 indigenous, and 412 cosmopolitan individuals in three slums in Southwestern Nigeria, health information and health-seeking behavior had higher prevalence data among cosmopolitan slum dwellers compared to their counterparts living in non-cosmopolitan slums [19]. A likely explanation for the findings in this study is the better coverage of COVID-19 information across social, print, and traditional media platforms in urban communities compared to rural populations. It is also likely that COVID-19 information is not tailored to suit the needs of rural residents, thus, the motivation to deliberately process and appraise the information may be lacking. Therefore, it is necessary that context-specific needs are introduced to design health messages as a strategy to improve COVID-19 health literacy especially among rural residents. Tailoring health information has been confirmed as a useful strategy towards enhancing information appraisal and promoting behavioral change [20].
Among the general adult population, this study found that rich people (fifth wealth quintile) had better COVID-19 health literacy compared to their poor counterparts (first wealth quintile). This finding could possibly be due to the limited sources of information available to the poor. The limited sources of information available to poor communities reduces their exposure to evidence-based COVID-19 information. The socioeconomic gradient in health literacy reported among the general population in this study is like the results of the HLS-EU survey which reported that health literacy is dependent on individuals’ socioeconomic status [4]. The findings in the present study are consistent with a cross-sectional study conducted in China which found that low income may negatively impact health literacy, thereby increasing the risk for poor health outcomes [21]. It could therefore be concluded from this study that there exists a pro-rich concentration in COVID-19 health literacy among the general adult population in Ondo State, Nigeria.
From this study, we found that older age was an important predictor of good COVID-19 health literacy among a cross-section of the population of Ondo State. In a cross-sectional study investigating the factors influencing health literacy across different age groups before and during the COVID-19 pandemic in Chongqing, China, it was reported that health literacy declined with increasing age [22]. Our findings in this study are in tandem with the findings of a cross-sectional study conducted among 1,030 adults in Mexico where older age was reported as a significant predictor of good health literacy [23]. In the present study, we identified the WHO as the most frequently consulted source of COVID-19 health information among community members in Nigeria. Updates on COVID-19 transmission, case fatality, and prevention are frequently communicated by the WHO across the internet. It is expected that a higher proportion of younger people have unlimited access to this information given their affinity for technology [24], however, it is older persons (aged >40 years) that have better COVID-19 health literacy. Strategies through which health organizations and media sources can improve the presentation of COVID-19 information to capture the interests of young people in Nigeria needs to be immediately considered.
From this study, living with someone in the COVID-19 high risk group was identified as a significant predictor of good COVID-19 health literacy in both rural and urban communities of Ondo State, Nigeria. Home-based care is a recommended strategy for providing care to COVID-19 positives within their homes and necessitates caregivers to be knowledgeable about COVID-19, its mode of transmission, and protection [25]. Thus, it is likely that many people living with someone in the COVID-19 high risk group (those aged ≥65 years) practice home-based care when these persons experience COVID-19 symptoms [26]. Thus, many people living with someone in the COVID-19 high risk group (those aged ≥65 years) may be less likely to be misinformed about COVID-19. To improve COVID-19 health literacy among the populace, health literacy should focus on all population groups to improve their access to relevant COVID-19-related information.
There are a few limitations to the present study. Firstly, the demographic structure of the subjects in this study does not represent that of the overall population in Nigeria [27]. While the population pyramid describes the demography within a 5-year interval (e.g., 0-4 years, 5-9 years…≥85years), this study included only adults (people aged ≥18 years). Thus, people who belong to the first three cohorts (0-4 years, 5-9 years, and 10-14 years) on the demographic pyramid were excluded, and only a marginal proportion of those in the 15-19 years cohort were included in this study. Secondly, this study was conducted in only one state in Nigeria, hence, the health literacy reported herein cannot be used to accurately represent that of the entire country. Thirdly, the survey was conducted in October 2020, thus, it is possible that COVID-19 health literacy has improved among the general adult population in Ondo State at the time this work was written.
This study found a higher prevalence of COVID-19 health literacy among urban dwellers compared to rural dwellers in Ondo State, Nigeria. Factors associated with COVID-19 health literacy among people living in urban communities included older age and living with a COVID-19 high risk group, while older age and upper wealth quintiles were associated with COVID-19 health literacy among rural residents. It is very likely that people living in rural areas have limited internet access compared to urban residents, a factor that limits their access to a range of sources of health information. Since COVID-19 is here to stay, integrating COVID-19 health literacy education into national health literacy programs could be an effective strategy in addressing urban-rural differences in COVID-19 health literacy. Health workers are one of the most important sources of COVID-19 health literacy in rural communities; nurse practitioners and local health departments should be engaged to provide rural residents with improved COVID-19 health literacy. This will require the development of health literacy content for dispensaries, community health clinics, and other local health facilities where community members receive healthcare. COVID-19 campaigns should also be presented in local languages to reduce existing rural-urban differences in COVID-19 health literacy.
The authors declare no conflicts of interest. This research did not receive any specific grant from any funding agency in public, commercial or not-for-profit sectors.
The authors are grateful to all community members in the study area for their participation in this study.
AAA conceptualized the study. Both OSI and AAA contributed equally to the design of the research, as well as the analysis, and writing of the manuscript. Both authors critically revised the manuscript and approved its final version.
1. Kotlar B, Gerson E, Petrillo S, Langer A, Tiemeier H. The impact of the COVID-19 pandemic on maternal and perinatal health: a scoping review. BMC Reproductive Health. 2021;18:10. https://doi.org/10.1186/s12978-021-01070-6.
2. World Health Organization. Vaccine efficacy, effectiveness, and protection [Internet]. [cited 2021 Dec 28]. Available from: https://www.who.int/news-room/feature-stories/detail/vaccine-efficacy-effectiveness-and-protection
3. Lastrucci V, Lorini C, Del Riccio M, Gori E, Chiesi F, Moscadelli A, Zanella B, et al. The Role of Health Literacy in COVID-19 Preventive Behaviors and Infection Risk Perception: Evidence from a Population-Based Sample of Essential Frontline Workers during the Lockdown in the Province of Prato (Tuscany, Italy). Int J Environ Res Public Health. 2021;18(24):13386. https://doi.org/10.3390/ijerph182413386.
4. Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, Brand H; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80. https://doi.org/10.1186/1471-2458-12-80.
5. Okoli C, Hajizadeh M, Rahman MM, Khanam R. Geographical and socioeconomic inequalities in the utilization of maternal healthcare services in Nigeria: 2003-2017. BMC Health Serv Res. 2020;20(1):849. https://doi.org/10.1186/s12913-020-05700-w.
6. Kuyinu YA, Femi-Adebayo TT, Adebayo BI, Abdurraheem-Salami I, Odusanya OO. Health literacy: Prevalence and determinants in Lagos State, Nigeria. PLoS One. 2020;15(8):e0237813. https://doi.org/10.1371/journal.pone.0237813.
7. Cross SH, Mehra MR, Bhatt DL, Nasir K, O'Donnell CJ, Califf RM, Warraich HJ. Rural-Urban Differences in Cardiovascular Mortality in the US, 1999-2017. JAMA. 2020;323(18):1852-1854. https://doi.org/10.1001/jama.2020.2047.
8. Zibima SB, Ennag K, Oniso JI, Moses EB. Health literacy level in rural Bayelsa, Nigeria’s Niger Delta Region. Int J Community Med Public Health. 2021;8(3):1115-1121. https://dx.doi.org/10.18203/2394-6040.ijcmph20210790
9. World Health Organization. Unmasking And Overcoming Health Inequities in Urban settings [Internet]. [cited 2022 Apr 24]. Available from: https://apps.who.int/iris/bitstream/handle/10665/44439/9789241548038_eng.pdf;sequence=1
10. Singh GK, Siahpush M. Widening rural-urban disparities in all-cause mortality and mortality from major causes of death in the USA, 1969-2009. J Urban Health. 2014;91(2):272-292. https://doi.org/10.1007/s11524-013-9847-2.
11. Huang J, Guan ML, Balch J, Wu E, Rao H, Lin A, et al. Survey of hepatitis B knowledge and stigma among chronically infected patients and uninfected persons in Beijing, China. Liver Int. 2016;36(11):1595-1603. https://doi.org/10.1111/liv.13168.
12. Britannica. Ondo State, Nigeria [Internet]. 2009 [cited 2020 Nov 26]. Available from: https://www.britannica.com/place/Ondo-state-Nigeria
13. Nigeria Center for Disease Control. 2020. COVID-19 Nigeria. Accessed on: 28 April 2022. Available from: https://covid19.ncdc.gov.ng/
14. Whitley E, Ball J. Statistics review 4: sample size calculations. Crit Care. 2002;6(4):335-341. https://doi.org/10.1186/cc1521.
15. IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.
16. World Medical Association. WMA Declaration of Helsinki – Ethical Principles For Medical Research Involving Human Subjects [Internet]. [cited 2022 Apr 28]. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
17. Chen X, Chen H. Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. Int J Environ Res Public Health. 2020;17(12):4437. https://doi.org/10.3390/ijerph17124437.
18. Onyeonoro UU, Ogah OS, Ukegbu AU, Chukwuonye II, Madukwe OO, Moses AO. Urban-Rural Differences in Health-Care-Seeking Pattern of Residents of Abia State, Nigeria, and the Implication in the Control of NCDs. Health Serv Insights. 2016;9:29-36. https://doi.org/10.4137/HSI.S31865.
19. Fayehun O, Ajisola M, Uthman O, Oyebode O, Oladejo A, Owoaje E, Taiwo O, Odubanjo O, Harris B, Lilford R, Omigbodun A. Improving Health in Slums Collaborative. A contextual exploration of healthcare service use in urban slums in Nigeria. PLoS One. 2022;5;17(2):e0264725. https://doi.org/10.1371/journal.pone.0264725.
20. Ukwenya VO, Fuwape TA, Ilesanmi OS. COVID-19 health literacy, coping strategies and perception of COVID-19 containment measures among community members in a southwestern state in Nigeria. GERMS. 2021;11(4):478-497. https://doi.org/10.18683/germs.2021.1284.
21. Tang C, Wu X, Chen X, Pan B, Yang X. Examining income-related inequality in health literacy and health-information seeking among urban population in China. BMC Public Health. 2019;19:221. https://doi.org/10.1186/s12889-019-6538-2.
22. Sánchez-Arenas R, Doubova SV, González-Pérez MA, Pérez-Cuevas R. Factors associated with COVID-19 preventive health behaviors among the general public in Mexico City and the State of Mexico. PLoS One. 2021;16(7):e0254435. https://doi.org/10.1371/journal.pone.0254435.
23. World Health Organization. Home care for patients with suspected or confirmed COVID-19 and management of their contacts. WHO; 2020. Available from: https://www.who.int/publications/i/item/home-care-for-patients-with-suspected-novel-coronavirus-(ncov)-infection-presenting-with-mild-symptoms-and-management-of-contacts.
24. Nigeria Centre for Disease Control. Interim Guidelines for Home Care of Confirmed COVID-19 Cases. NCDC; 2020. Available from: https://covid19.ncdc.gov.ng/media/files/HomeCareInterimGuide.pdf
25. Ilesanmi OS, Afolabi AA. A scope review on home-based care practices for COVID-19: What Nigeria can learn from other countries. Ibom Med J. 2021;14:1-9.
26. Yang P, Ou Y, Yang H, Pei X, Li J, Wang Y, Tan F, Zhao X, Liu W. Research on Influencing Factors and Dimensions of Health Literacy in Different Age Groups: Before and After the COVID-19 Era in Chongqing, China. Front Public Health. 2021. https://doi.org/10.3389/fpubh.2021.690525.
27. PopulationPyramid.net. Population Pyramids of the World from 1950 to 2100 [Internet]. 2019 [cited 2022 Jul 28]. Available from: https://www.populationpyramid.net/nigeria/2019/